case of 45 years old man
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs. This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box.
A 45 year old man presented to the casualty on 2/11/21 with the complaints of Fever since 4 days
Body pains since 4 days
Reduced urine output since 3 days
Vomiting yesterday
Hematuria since morning
Black tarry stools since morning
High grade fever, intermittent,not associated with chills and rigors .
2 episodes of non projectile, non bilious, blood tinged vomiting yesterday
He was taken to an outside hospital where in he received fluids and later the attenders decided to pay a visit to our hospital.
Hematuria since morning
1 episode of black tarry stool in the morning
He is a farmer by occupation and He works at the daily farm . His wife works as a farmer as well. His wife was previously admitted with us with ?meningitis. He has 2 children.
He is an alcoholic since the past 20 years with around 90 ml of whiskey everyday. His last intake of whiskey was 4 days. He smokes around 2 packs of beedi everyday since the past 20 years.
1 year back he presented to our hospital with the complaints of pain abdomen after which he underwent an abdominal surgery.
Since the past 4 years he has been experiencing high grade fever, intermittent with no diurnal variation associated with pain in his thigh muscles and arm.
Reduced urine output since morning
On presentation he is a thin built individual
Subconjunctival hemorrhage +
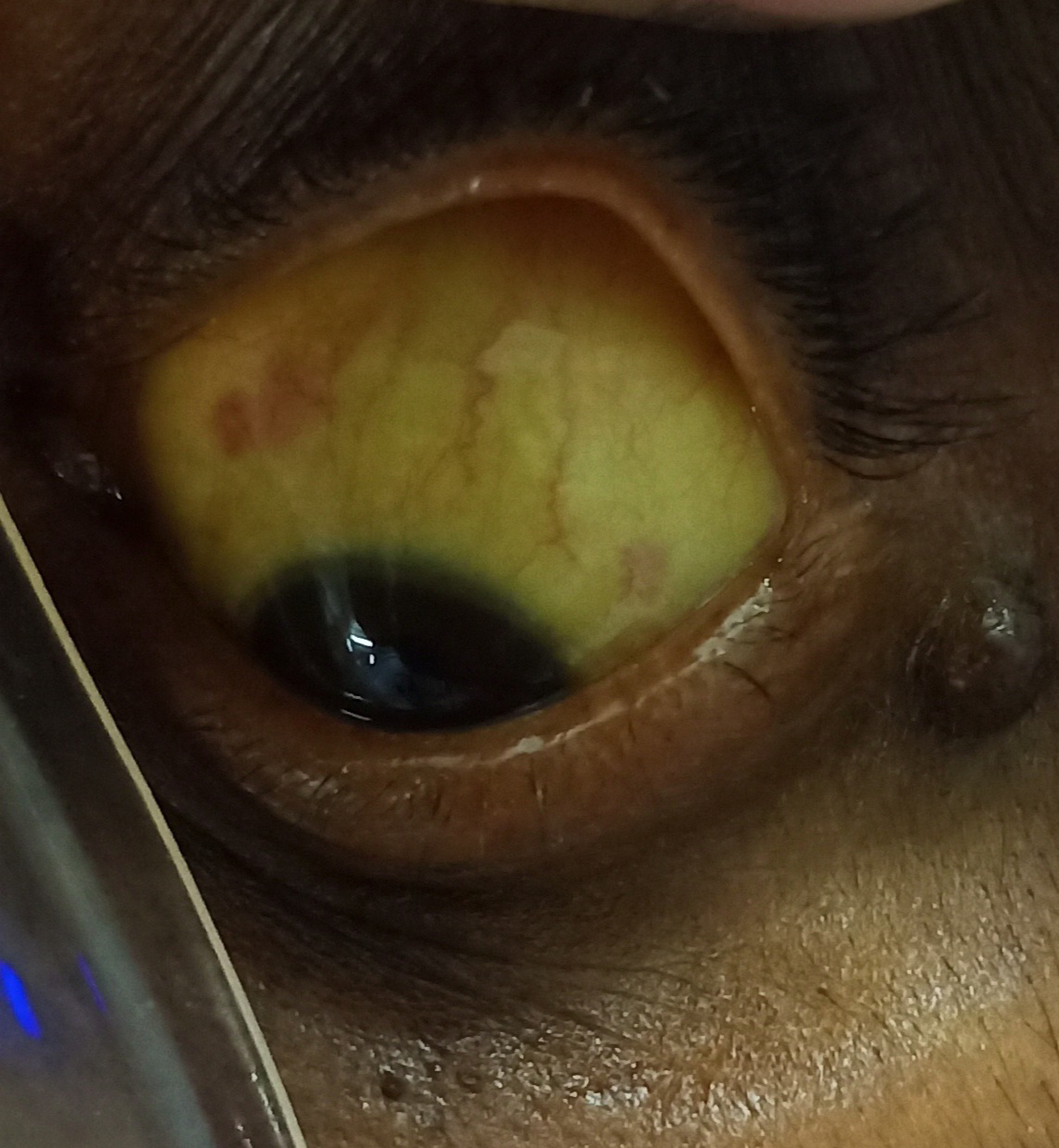
Icterus+
Pallor +
Clubbing +
Image of right eye showing icterus
Images of left eye showing sub conjuctival haemorrhage


Image showing yellowish discolouration of nails and clubbing

Bp was 60mmhg on palpation
PR - 115bpm
RR - 25 cpm
Spo2 - 92% on Room air
Afebrile
Lungs -
Inspiratory crepitations in Bilteral IAA,ISA

4/11/21 xray chest

7/11/21 chest xray

8/11/21 chest xray



Cvs - S1,S2+
Per Abdomen -
Soft
Nontender

HB - 8 ( outside 2 days back 11g/dl)
TLC - 8400
Plt - 15,000
Total Bilirubin - 11
Direct Bil - 7.05
Ast - 327
Alt - 187
Alp - 303
Albumin - 2.4
Serum creatinine - 2.5
Blood urea - 82
Dengue negative
Abg showing metabolic acidosis with PH 7.32
Hco3 - 9
Pco2 - 19
Po2 - 101 with oxygen on 6L of O2
Diagnosis -
Septic Shock with MODS secondary to ? Leptospirosis
Pyrexia with bicytopenia
Direct hyperbilirubinemia and prerenal AKI
3/11/21
In view of low platelet count of 14,000 sdp transfusion is planned.
After doing cross matching a screened unit of sdp is issued to the patient for transfusion after taking consent from the patient attenders.
Post transfusion the platelet count is improved to 35000.
4/11/21
S- patient is complaining of, productive cough with hemoptysis ,
chest pain - non radiating , burning type ,
Increasing on coughing and taking deep inspiration
O- icteric,pallor, subconjunctival hemorrhage
PR-112
BP- 110/80 mmhg on Noradrenaline -16 ml /hr
RR- 36/min
Spo2- 99% of
RS- BAE present ,crepts over left infraxillary ,infrascpular regions .
CvS- S1, S2 heard
P/ A soft
Urine output - increased
I/O - 3200/1300 ml
A- Septic shock secondary to leptospirosis ( Pre Renal AKI - resolving
Pyrexia with bicytopenia
Hypoxia + - secondary to ARDS?
P- Oxygen supplementation @14 litres/ min to maintain spo2 more than 95%
Iv fluids
Inj . ceftriaxone 1gm / IV/BD
Inj.doxy 100 mg / IV/BD
TEMP charting ,vitals monitoring
This case is intubated in view of respiratory failure..on 4/11/21
ABG shows
pO2:-41
FiO2:-60
Patient ET tube blocked with blood clot .
Even after mucomist,ambu and suction saturations weren't improving .
Removed and placed a new tube.
During which patient had Bradycardia ,hypoxia and absent central and peripheral pulses ,
3 cycles of CPR done , patient revived .
Post CPR vitals -
Pupils -
PR-112/ min ,regular
Bp-110/80 mmHg
RS - BAE + , bilateral diffuse crepetations +
CVS-s1 ,S2 heard
Spo2-100% with Fio2-80 %
ABG - severe acidosis mixed metabolic and respiratory -acidosis
Image showing chest xray post reintubation

5/11/21
2 units of FFP is transfused after doing crossmatching.Consent was obtained for transfusion from the patient attenders and transfusion done
Day 2 of mechanical ventilation .
Patient is becoming conscious intermittently ,with eye openings to painful stimuli and verbal commands .
Fever spikes present .
O- Pt onmechanical ventilation -AcMV - VC mode
With RR- 33/ min
Peep - 7
VT-400 ml
Fio2-21 %
icteric,pallor, subconjunctival hemorrhage
Pupils - normal size ,non reacting to light
Afebrile
PR-97/ min ,regular
BP- 120/80 mmhg
Spo2- 94% with fio2-21%
RS- BAE present ,bilateral crepts + infraxillary ,infrascpular regions .
CvS- S1, S2 heard
P/ A soft
Urine output - increased
A- MODS- weils syndrome
P-
Iv fluids
Inj . ceftriaxone 1gm / IV/BD
Inj.doxy 100 mg / IV/BD
TEMP charting ,vitals monitoring.
Weaning sedation .
Plan to - Shift to CPAP mode
7/11/21
Extubation done at 01:00pm on 7/11/21
Under all aseptic precations,with premedication inj.HYDROCORT 100MG IV STAT and nebulisation with BUDECORT and MUCOMIST , extubation was done. Procedure was uneventful and post extubation vitas are stable.
Bp :120/70mmhg
Pr :108bpm
Spo2 : 98% On 10L of O2
Cvs : s1 s2 heard
RS : BAE present
P/A :soft and nontender
GCS : E4V5M6
Day 1 after extubation
weils syndrome MODS
S- patient is having fever spikes , cough with sputum yellow coloured,non blood stained ,shortness of breath , generalized bodypains .
Yesterday night - patient had one episode of high grade fever with chills ,became tachypneic .
Connected to NIV - CPAP.
O- ABG with high flow oxygen showed Hypoxia ,hence
Patient was on CPAP PC mode overnight
With RR- 33/ min
Peep - 7
Fio2-50%
icteric,pallor, subconjunctival hemorrhage
Afebrile
PR-90/ min ,regular
BP- 130/90 mmhg
RR-37 / min
Spo2- 100% with fio2-80%
RS- BAE present ,bilateral crepts + infraxillary ,infrascpular regions .
CvS- S1,S2 heard
P/ A soft
A-
1-MODS- weils syndrome
2- ARDS?
P-
Iv fluids
Inj . ceftriaxone 1gm / IV/BD
Inj.doxy 100 mg / IV/BD
TEMP charting ,vitals monitoring.
In view of persistent fever spikes ,hypoxia , tachypnea,new radiological opacties -Emperical antibiotic coverage for VAP was started with levofloxacin and vancomycin .
8/11/21
weils syndrome MODS
S- patient is having fever spikes , cough with sputum yellow coloured,non blood stained ,shortness of breath , generalized bodypains .
Yesterday night - patient had one episode of high grade fever with chills ,became tachypneic .
Connected to NIV - CPAP.
O- ABG with high flow oxygen showed Hypoxia ,hence
Patient was on CPAP PC mode overnight
With RR- 33/ min
Peep - 7
Fio2-50%
icteric,pallor, subconjunctival hemorrhage
Afebrile
PR-90/ min ,regular
BP- 130/90 mmhg
RR-37 / min
Spo2- 100% with fio2-80%
RS- BAE present ,bilateral crepts + infraxillary ,infrascpular regions .
CvS- S1,S2 heard
P/ A soft
A-
1-MODS- weils syndrome
2- Ventilator Associated pneumonia ?
P-
Iv fluids
Inj . ceftriaxone 1gm / IV/BD
Inj.doxy 100 mg / IV/BD
TEMP charting ,vitals monitoring.
In view of persistent fever spikes ,hypoxia , tachypnea,new radiological opacties -Emperical antibiotic coverage for VAP was started with levofloxacin and vancomycin .
9/11/21
S- patient is having fever spikes , cough with sputum yellow coloured,non blood stained ,shortness of breath , generalized bodypains .
O- Febrile- Temp -102
icteric,pallor, subconjunctival hemorrhage
PR-122/ min ,regular
BP- 120/80 mmhg
RR-46 / min
Spo2- 92 % with high flow oxygen -14 litrs
RS- BAE present ,bilateral crepts + infraxillary ,infrascpular regions .
CvS- S1,S2 heard
P/ A soft
I/o -5500/2750 ml
A-
1-MODS- weils syndrome
2- Ventilator Associated pneumonia ?
P-
Iv fluids
Inj . ceftriaxone 1gm / IV/BD
Inj.doxy 100 mg / IV/BD
Inj.Meropenam 1gm /IV/BD
Intermittent CPAP
TEMP charting ,vitals monitoring.
10/11/21
weils syndrome MODS
S- patient is having fever spikes , cough with sputum yellow coloured,non blood stained , severe shortness of breath- , generalized bodypains .
He is dependant on CPAP ,
With high flow oxygen - sats -80 % and low
With CPAP -fio2 100%
O- Febrile- Temp -101
icteric,pallor, subconjunctival hemorrhage
PR-110/ min ,regular
BP- 120/80 mmhg
RR-46 / min
Spo2- 99 % with CPAP PC mode ,fio2-100 %
RS- BAE present ,bilateral crepts + , inframammary infraxillary ,infrascpular regions .
CvS- S1,S2 heard
P/ A soft
A-
1-MODS- weils syndrome
2- Ventilator Associated pneumonia
P-
Iv fluids
Inj . Colistin 2.5 MIU / iv /Stat given .
Inj.doxy 100 mg / IV/BD
Inj.Meropenam 1gm /IV/BD
Continuous CPAP mode
TEMP charting ,vitals monitoring.
11/11/21
weils syndrome MODS
VAP
S- patient is having fever spikes .
Complaining of Shortness of breath even on CPAP with 100% FIo2 .
O- Febrile- Temp -102 F
icteric,pallor, subconjunctival hemorrhage
PR-130/ min ,regular
BP- 130/80 mmhg
RR-34 / min
Spo2- 90 % with CPAP PC mode ,fio2-100 %
PEEP- 10 cm
Pinsp-20
RS- BAE present ,bilateral diffuse crepts +
CvS- S1,S2 heard
P/ A soft
A-
1-MODS- weils syndrome
2- Ventilator Associated pneumonia - Multi drug resistant gram negative bacteria ( klebsiella , acinetobacter )
P-
Iv fluids
Inj . Colistin 2.5 MIU / iv /BD .
Inj.Amikacin 1000 mg/IV/OD
Inj.doxy 100 mg / IV/BD
Inj.Meropenam 1gm /IV/BD
Continuous CPAP mode
TEMP charting ,vitals monitoring.

He might get intubated again .
CPR NOTES
IN VIEW OF FALL IN SATURATIONS WITH NO CENTRAL AND PERIPHERAL PULSES AND BPBNOT RECORDABLE AN IMMEDIATE CPR IN INITIATED ACCORDING TO ACLS GUIDLINES
11:00 AM BP/PR NOT RECORDABLE CPR STARTED 1 CC ADRENALINE GIVEN
CPR WAS CONTINUED TILL 11:35 AM WITH 1 CC ADRENALINE EVERY 5 MINS STILL BP AND PR NOT RECORDABLE AND CPR STOPPED
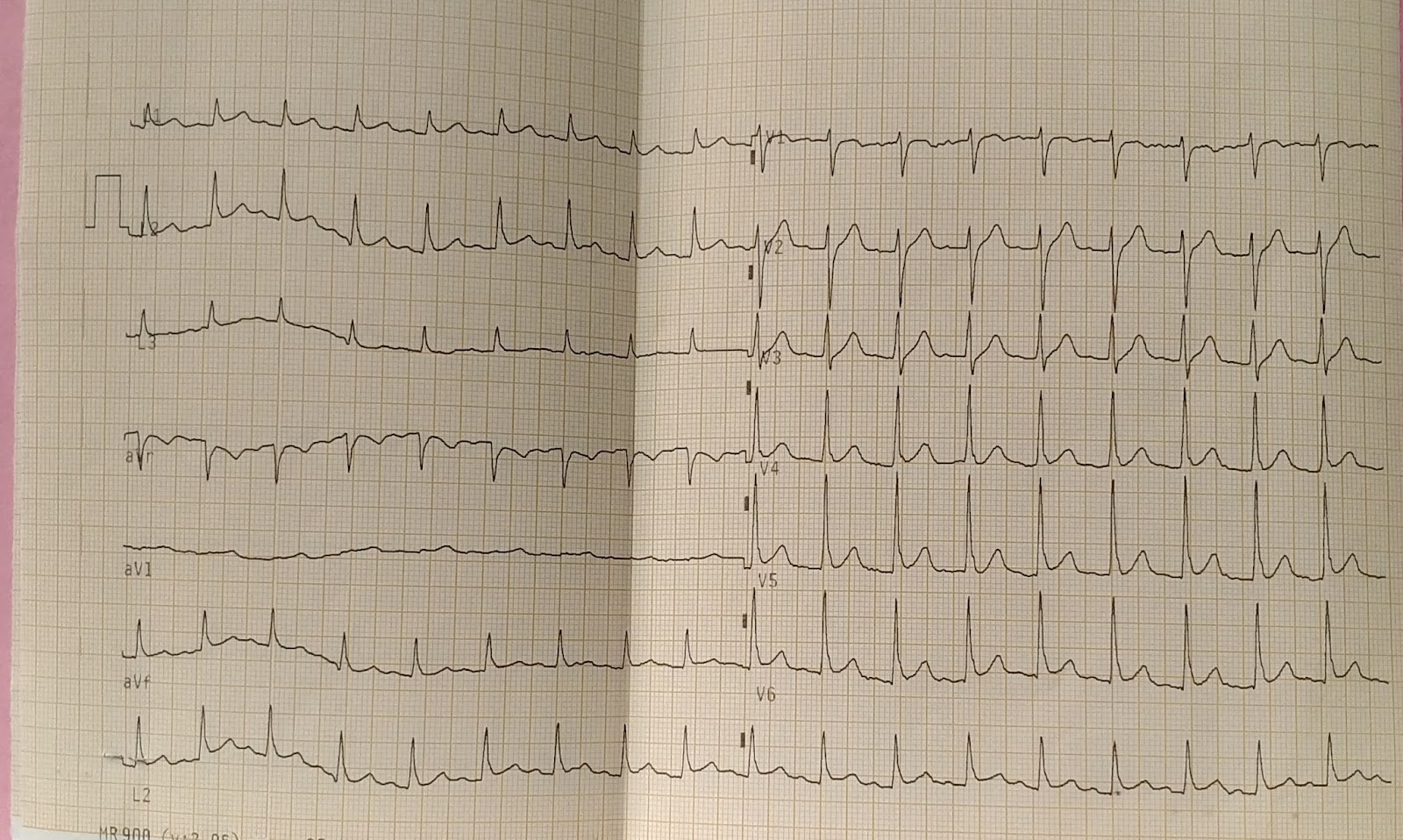
INSPITE OF ALL THE ABOVE RESUSCITATIVE EFFEORTS THE PATIENT COULDN'T BE REVIVED BACK AND ECG SHOWS FLAT LINE AND DECLARED DEATH ON 11/11/21 AT 11:36 AM
CAUSE OF DEATH: VENTILATOR ASSOCIATED PNEUMONIA , SEVERE ARDS,DIFFUSE ALVEOLAR HEMORRHAGES , SEPTIC SHOCK WITH MODS 2° TO LEPTOSPIROSIS
Death notes :-
45 YAER OLD KALE PATIENT DIAGNOSED WITH SEPETIC SHOCK WITH MODS 2° TO LEPTOSPIROSIS SEVERE ARDS 2° TO ? VENTILATORY ASSOCIATED PNEUMONIA ? DIFFUSE ALVEOLAR HEMORRHAGE ON 11/11/21 AT 11:00 AM PATIENT SUDDENLY BECAME UNCONSCIOUS WITH BP AND PULSE NOT RECORDABLE ,AN IMMEDIATE CPR IS INITIATED ACCORDING TO ACLS GUIDLINES . PATIENT WAS RE INTUBATED WITH FT NO 7.0 AND ADEQUATE RESUSCITATION WAS DONE INSPITE OF ALL THE ABOVE RESUSCITATIVE EFFORTS PATIENT COULDN'T REVIVED AND DECLARED DEAD ON 11/11/21 AT 11:36 PM
IMMEDIATE CAUSE:
1. SEVERE ARDS 2° TO VENTILATOR ASSOCIATED PNEUMONIA
ATECEDENT CAUSE: 2.SEPTIC SHOCK WITH MODS 2° TO LEPTOSPIROSIS
Day wise ABG reports
2/11/21 , 8.36pm

3/11/21 , 9.51 am

4/11/21 , 12.07pm

4/11/21, 1.28pm

4/11/21 , 6.12pm

4/11/21 , 10:23pm

5/11/21 , 08:30am

5/11/21 , 12.18pm

5/11/21 ,5.26 pm

6/11/21 , 3:19 pm

6/11/21 , 11:09 pm

7/11/21, 2:14pm

7/11/21 , 7:41 pm

7/11/21 , 10:34pm



Comments
Post a Comment