A case of 39 year old male
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs. This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box.
39yrs od male came with complaints of pain abdomen since 4 days.complaints of increased frequency of urination with burning micturition since 4 days,fever since 4 days.
Patient was apparently asymptomatic 3 yrs back then he went to a hospital with complaonts of increased frequency of urination and diagnosed to be as Type2 diabetes mellitus(and started on OHD's),he was on regular followup.Since 1 month he is on routine checkup.Had uncontrolled sugars >300.Now presented with complaints of pain abdomen at umbilicus and at lower abdomen region since 4 days
C/O b/l loin pain since 4 days,intermittent not associated with nausea ,vomiting,abdominal distension,loose stools.Burning micturition since 4 days with red colored urine.
C/O increased frequency of urination/urgency.Sometimes he is passing urine in his clothes before reaching the washroom (? Urge incontinence)
Fever since 4 days,low grade,intermittent, not associated with cough,cold.Not associated with chills and rigors.
No Shortness of breath
No palpitations
No pedal edema
On examination
No pallor , icterus , cyanosis , clubbing, lymphadenopathy , edema.
Temp : 100*F
Pulse : 86bpm
RS : 20cpm
BP : 150/100mmhg
Spo2 : 98% at RA
GRBS : 274mg/dl
CVS : S1,S2 heard
RS : BAE present.NVBS
P/A : Tenderness present at lower abdominal region,B/L loin tenderness present
CNS : No focal neurological deficet
Provisional diagnosis :
?Acute pyeonephritis
? Acute cystitis
K/c/o diabetes mellitus type 2 since 3 years

ECG:-

USG abdomen


17/11/21
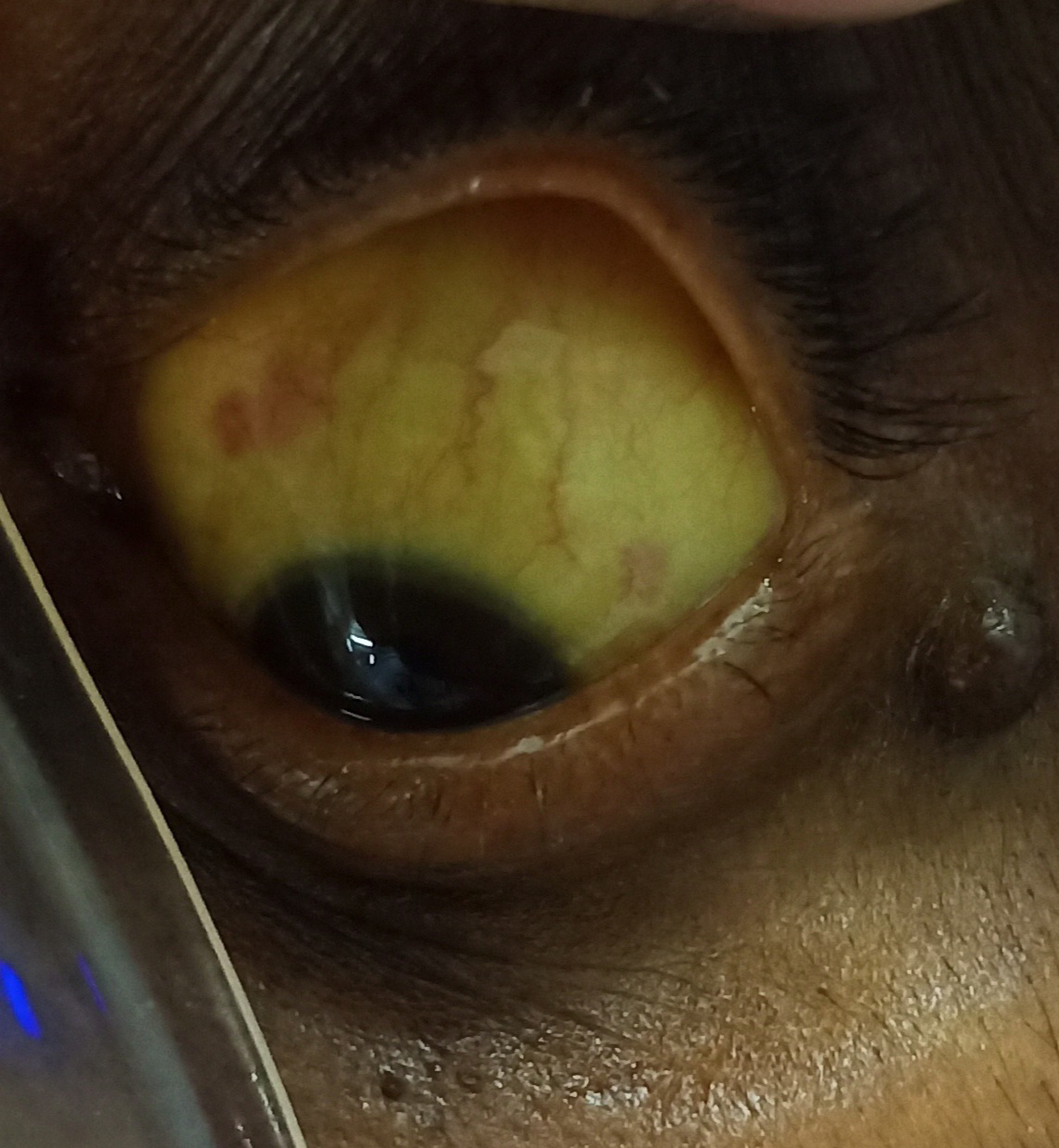
Ophthal referal was done to rule out diabetic retinopathy as the patient is a k/c/o diabetes mellitus type 2 since 3 years.

Review USG

2D ECHO

18/11/21
Soap notes :-
S-
Burning micturition reduced
C/O pain abdomen decreased
O -
Bp -130/90mmhg
Pr- 87bpm
temp - 99F
spo 2 -96% at RA
A-
? Acute pyelonephritis
?cystitis
known case of DM type 2 and denovo HTN
P -
1.IVF NS/RL @ 100ml/hr
2.INJ.PIPTAZ 4.5 gm/IV/BD
3.INJ.ZOFER 4mg/TID
4.INJ.HA1 S/C ACC TO SLIDING SCALE
5.INJ.OPTINEURON 1 amp in 100ml NS
6.TAB.PCM 650mg PO SOS
7.Tab.AMLONG 5mg OD
8.STRICT I/O CHARTING
9.GRBS Monitoring 6th hourly
10.Bp/pr/temp monitoring 4th hourly
19/11/21 :-
S
c/o Burning micturition present
Fever spikes +
Increased frequency of urination
O
BP- 130/80 MMHG
TEMP-100 ° F
PR- 88 BPM
CVS - S1S2 +
RS - BAE +
P/A- Soft ,non tender
CNS- NO FND
GRBS-151 mg/dl
I/O - 2000/1250
A
? ACUTE PYELONEPHRITIS /? CYSTITIS
K/C/O DM AND DENOVA HTN
P
TAB. CIPROFLOXACIN 500MG PO BD
TAB PAN 40 MG PO OD
INJ HAI S/C ACC TO GRBS
(BBF-BL-BD)
TAB PCM 1000MG PO QID
TAB AMLONG 5MG PO OD
GRBS 5TH HOURLY
MONITORING VITALS
SYP CITRALKA 10 ML IN 1GLASS OF WATER PO OD
TAB URISPAS PO BD

20/11/21
39 years male
AMC bed 1
S-
Burning micturition reduced
C/O pain abdomen decreased
C/O fever
O -
Bp -110/70mmhg
Pr- 89bpm
temp - 100F
spo 2 -98% at RA
A-
? Acute pyelonephritis
?cystitis
known case of DM type 2 and denovo HTN
P -
1.IVF NS/RL @ 100ml/hr
2.INJ.ZOFER 4mg/TID
3.INJ.HA1 S/C ACC TO SLIDING SCALE
4.INJ.OPTINEURON 1 amp in 100ml NS
5.TAB.PCM 1g 6 hrly
6.Tab.AMLONG 5mg OD
7.STRICT I/O CHARTING
8.GRBS Monitoring 6th hourly
9.Bp/pr/temp monitoring 4th hourly
21/11/21
S
- Continuous fever spikes present above 102 F associated with chills
C/o burning micturation subsides and increased frequency of urination,low backache increased on bending forward
O- TEMP-101F
Bp-110/70mmhg
Pr-90bpm
Cvs-s1,s2heard
Rs- NVBS
CNS-NAD
A
- Diagnosis is ? Acute pyelonephritis and urge incontinence .
Dm-2
?clinical malaria
Urine c/s - no growth
Sent repeat blood and urine c/s
Smear for mp - negative.
Repeat cue - no RBC casts and pus cells -8-10 .
Xray kub was done in view of ??emphysematous pyelonephritis .
P
1.Tab.CIPROFLOXACIN 50MG /BD
2.Tab.PAN 40MG OD
3.TAB.PCM 650mg QID
4.Tab.AMLONG 5mg PO OD
5.Tab.URISPAS PO BD
6.INJ.HUMAN INSULIN
7.Syp.CITRALKA 10ML IN ONE GLASS WATER POBD
8.GRBS MONITORING
9.INJ.FALCIGO 120MG IV STAT
10.BP/PR/TEMP MONITORING
22/11/21
S- no fever spike since 4pm yesterday, pt is feeling less lethargic, good appetite,
lowbackache+
no burning micturition
O- TEMP-98.6F
Bp-120/70mmhg
Pr-90bpm
Cvs-s1,s2heard
Rs- NVBS
CNS-NAD
A
- Diagnosis is ? Acute pyelonephritis and urge incontinence .
Dm-2
?clinical malaria
haemogram awaited
P
1.inj meropenem 1gm/iv/bd
2.Tab.PAN 40MG OD
3.TAB.PCM 650mg QID
4.Tab.AMLONG 5mg PO OD
6.INJ.HUMAN INSULIN nph 6----6,regular 6---6---6
7.Syp.CITRALKA 10ML IN ONE GLASS WATER POBD
8.GRBS MONITORING
9.INJ.FALCIGO 120MG IV 8pm today
10.BP/PR/TEMP MONITORING
23/11/21
S- loin pain+ but decreased,no burning micturition, chills at the time of fever spike, less lethargic,
last spike at 8 pm yesterday.
O- TEMP-98.6F
Bp-120/80mmhg
Pr-90bpm
Cvs-s1,s2heard
Rs- NVBS
CNS-NAD
A
- Diagnosis is UTI
Dm-2
?clinical malaria
P
1.inj meropenem 1gm/iv/bd
2.Tab.PAN 40MG OD
3.inj neomol 1gm/iv/tid
4.Tab.AMLONG 5mg PO OD
6.INJ.HUMAN INSULIN nph 8----8,regular 8---8---8
8.GRBS MONITORING
9.INJ.FALCIGO 120MG IV 8am today.
10.BP/PR/TEMP MONITORING
24/11/21
S-
No Burning micturition
Lower bacheache decreased
O -
Bp -130/70mmhg
Pr- 88bpm
temp - 100F
spo 2 -98% at RA
A-
? Acute pyelonephritis
?cystitis
? Clinical malaria
? Acute prostatitis
known case of DM type 2 and denovo HTN
P -
1.Tab. FEROPENEM 200MG BD
2.Tab.DOXYCYCLINE 100MG PO OD
3.TAB PCM 650MG PO TID
4.INJ.HA1 S/C ACC TO SLIDING SCALE
5.TAB.PAN 40MG PO OD
6.Tab.AMLONG 5mg OD
7.STRICT I/O CHARTING
8.GRBS Monitoring 6th hourly
9.Bp/pr/temp monitoring 4th hourly

Comments
Post a Comment